Review Article
March 2025, 34:1
First online: 04 March 2025
Review Article
Coronary CT Angiography and Percutaneous Coronary Intervention: a Short Perspective from Interventional Cardiologist
Sidhi Laksono 1, 2 ,3
2 Division of Cardiac Imaging, Department of Cardiology and Vascular Medicine, Siloam Heart Center, Cinere, Depok, Indonesia
3 Faculty of Medicine, Universitas Muhammadiyah Prof Dr Hamka, Tangerang, Indonesia
Corresponding and main author: sidhilaksono@uhamka.ac.id
ABSTRACT
Coronary CT angiography (CCTA) is currently acknowledged as a successful non-invasive technique for detecting coronary artery disease (CAD) in stable angina patients. In addition to identifying CAD and assessing stenosis severity, CCTA now allows for the identification and characterization of plaques, size of lesions, and morphology of stenosis, while also aiding in the assessment of the physiological impact of stenosis using CT myocardial perfusion imaging and CT-based fractional flow reserve and potentially predicting the outcome of revascularization. CCTA’s distinctive feature is its ability to help with referring for invasive coronary angiography and facilitating in planning coronary intervention. This review discusses current and future applications of CCTA for percutaneous coronary intervention preparation, advocates for increased utilization of CCTA by interventional cardiologists, and explores how CCTA can improve patient care and clinical outcomes.
Keywords
CCTA, morphology, characteristic, CT-based noninvasive
functional imaging
INTRODUCTION
Coronary CT angiography (CCTA) is now a recognized primary non-invasive imaging technique to assess patients with suspected, but not confirmed, coronary artery disease (CAD).1 The current guidelines emphasize the strong ability of CCTA to rule out obstructive coronary stenosis due to its high negative predictive value.2 Recent advancements in CT systems and postprocessing techniques have led to the emergence of CT-based noninvasive functional imaging methods, including CCTA- fractional flow reserve computed tomography (CCTAFFRCT) and CT myocardial perfusion imaging, for the functional evaluation of CAD. The addition of FFRCT with stress-dynamic computed tomography perfusion (CTP) has demonstrated potential for enhancing the precision of CCTA in assessing stable chest discomfort and correlates with clinical outcomes.3 Furthermore, detecting atherosclerosis through CCTA offers valuable prognostic data for determining cardiovascular risk and informing treatment strategies. In the past ten years, the evaluation of the hemodynamic importance of CAD has been confirmed through CT-derived fractional flow reserve (FFRCT) and implemented in clinical settings to more accurately assess the physiological impact of each lesion and effectively identify patients who may require revascularization or whose need for invasive coronary angiography (ICA) can be delayed.4
In addition to its diagnostic accuracy, CCTA offers additional information that can be valuable in clinical settings for directing referrals to ICA and aiding in the planning of coronary interventions. Incorporating CCTA into the procedural planning of patients being considered for an invasive evaluation may help streamline the process of ICA, boost diagnostic and therapeutic measures, and enhance overall clinical results.5 With CCTA being increasingly used in assessing symptomatic patients, it is crucial to utilize existing data instead of ordering extra tests when planning and guiding coronary interventions. This review offers practical suggestions for incorporating CCTA into planning percutaneous coronary intervention (PCI) procedures.
Advancing the Significance of Utilizing CCTA Imaging in PCI
PCI is the most commonly used procedure for treating symptomatic CAD, in addition to optimal medical therapy. Advances in technology and next-generation drug-eluting stents have greatly enhanced patient results and reduced device-related issues.6 Unlike structural heart interventions, patients undergoing catheterization procedures often lack detailed information about their coronary anatomy and lesion characteristics. Coronary interventions are still carried out without noninvasive imaging beforehand to assist in treatment planning.7 This demonstrates a historical method because ICA was implemented before CCTA and ICA has been used for a long time without any additional anatomical imaging techniques. Inaccurate evaluation of lesion length and suboptimal fluoroscopic view angle may result in incomplete plaque coverage, leading to improper stent choice and increased adverse event rates.8 Additionally, plaques containing a high amount of calcium can result in insufficient stent expansion and increased occurrences of target vessel failure following PCI. Furthermore, low-attenuation plaques have been recognized as predictors of abnormal translesional physiology and periprocedural myocardial infarction. Therefore, CCTA offers additional details to ICA regarding the composition and volume of atherosclerotic plaque that may affect the invasive procedure.9
CCTA is a great tool for evaluating bypass grafts, as they are typically larger than coronary arteries and less affected by motion artifacts, particularly venous grafts. Similarly, CCTA plays a crucial role in evaluating the risk-to-benefit balance of the chronic total occlusion (CTO) PCI process.10 Moreover, CCTA’s role in clinical practice extends beyond just epicardial atherosclerotic CAD to include other clinical conditions like (high-risk subsets of coronary disease (left main and multivessel coronary disease), abnormal location and orientation of the coronary ostia, tortuosity, coronary fistulas and coronary aneurysms.11 For interventional cardiologists, CCTA can help in various ways during interventions, such as assisting in patient selection, catheter selection, optimizing workflow in the cardiac catheterization lab, and enhancing diagnostic accuracy and procedural safety.12 This evaluation examines particular clinical situations and emphasizes the important function of CCTA in helping cardiologists in day-to-day clinical settings.
On the other hand, the diagnostic efficacy of CTA is negatively correlated with the presence and severity of coronary artery calcium. Recognizing the constraints of CTA in patients with significant coronary calcification, several doctors choose to acquire a coronary calcium score to evaluate the efficacy of CTA in assessing CAD for each patient. The diagnostic efficacy of CTA is negatively correlated with the presence and severity of coronary artery calcium. Recognizing the constraints of CTA in patients with significant coronary calcification, several physicians choose to acquire a coronary calcium score to evaluate the efficacy of CTA in assessing CAD for each patient. In individuals with significant coronary calcification, CTP demonstrated diagnostic accuracy comparable to that of CTA. Nevertheless, CTP demonstrated incremental accuracy in the identification of hemodynamically significant stenosis, despite the fact that CTA was anomalous in all patients with a CAC score of over 400.13
Other studies indicate that the combination of coronary CTA and myocardial CTP demonstrates superior diagnostic performance compared to CTA alone in detecting coronary in-stent restenosis (ISR) and CAD. The combined CTA/CTP demonstrated an accuracy of 87% for the detection of ISR and 86% for CAD at the patient level, highlighting its strong diagnostic performance. In comparison to other prevalent noninvasive imaging modalities, including myocardial single-photon emission CT, cardiac magnetic resonance imaging, and stress echocardiography, CTP alone may lack sufficient accuracy to reliably exclude ISR. Conversely, CTA/CTP demonstrated significantly greater accuracy than stress tests.14
Morphology and Characterization of Coronary Lesion
Although there is a strong emphasis on lifestyle changes, controlling risk factors, and medication in cardiovascular disease guidelines, there is not enough focus on PCI planning and procedural technique.15 Failure to plan before a procedure can result in missing important factors, resulting in inaccurate assessment of coronary anatomy and atherosclerotic lesions,16 and improper selection of equipment and revascularization techniques. Even though optical coherence tomography and intravascular US offer valuable data on lesion characteristics and post-PCI stent implantation outcomes, their invasive, expensive, and time-consuming nature has limited their widespread adoption. Anatomical, non-invasive assessment using CCTA enables a detailed analysis of both the quality and quantity of coronary arteries, offering insights into plaque features, vessel size, and extent of lesions.17
One important goal in enhancing procedural success and patient outcomes is making sure that all plaques are fully covered. Incomplete coverage of plaque in a diseased segment is linked to a higher risk of target-vessel revascularization and a threefold rise in myocardial infarction within the first year. CCTA’s capability to accurately assess lesion length can be used in advance preparation for PCI, providing a full view of the coronary vasculature with none of the issues of foreshortening and overlapping commonly seen with invasive angiography.18 Vessel overlap, foreshortening, and beam attenuation are key obstacles in accurately assessing coronary anatomy during ICA, potentially causing underestimation of lesion dimensions, especially when evaluating side-branch ostium in bifurcation lesions. The 3D capability of CCTA enables precise evaluation of bifurcation lesion size and plaque location in relation to the carina, which can help determine the best viewing angles.19 These visual representations can be helpful for intricate lesions like unprotected stenosis in the left main coronary artery. Furthermore, detecting patients with left main disease prior to the invasive procedure can help with determining the best revascularization method, obtaining patient consent, and preparing for possible use of hemodynamic support devices.20
CCTA not only evaluates the inside of the arteries but also assesses the characteristics of coronary lesions and plaque features, showing good agreement with intravascular imaging US.21 Atherosclerotic plaques can be categorized based on Hounsfield units into calcified, noncalcified, or mixed types. Identifying coronary plaque composition is crucial for predicting plaque stability. Therefore, precise recognition of coronary plaque characteristics on CCTA could serve as a useful method for identifying patients at higher risk for coronary events during and after procedures. Calcified plaques are lesions that have a high CT value (>320 HU). Severely calcified blockages in coronary arteries can make stent placement difficult and, if not properly addressed, result in inadequate expansion of the stent.22, 23 Stent failure in the short and midterm follow-up is frequently due to underexpansion of the stent. Assessing the calcium arc, length, and thickness before a procedure is important for planning and guiding PCI.24
The presence of a circular calcium ring on CCTA may lead the interventional cardiologist to think about preparing the lesion to break up the calcium deposit to help the stent expand. In contrast, if no concentric calcifications and short calcific plaque are present, using a high-pressure noncompliant balloon for PCI would be enough to ensure optimal stent expansion. The primary drawback of CCTA for evaluating calcified plaque is its inability to pinpoint the location of the calcium within the vessel wall (i.e., superficial versus deep). The position of the calcium is important for treatment because rotational and orbital atherectomy are effective in treating cases where calcium is close to the surface.25
Noncalcified plaques are recognized as separate factors that can predict the occurrence of periprocedural no-reflow phenomenon and myocardial infarction.26 Besides determining if a plaque is calcified or noncalcified, CCTA can identify distinct features of high-risk plaques such as positive vessel remodeling, low attenuation plaque, spotty calcification, and napkin-ring sign. These characteristics add predictive value beyond just the stenosis and atherosclerotic burden level and are linked to abnormal translesional physiology. This emphasizes the significance of detecting high-risk plaque characteristics before ICA, particularly in mild to moderate stenosis cases where translesional physiology can help inform treatment choices through invasive FFR measurements.27
Coronary flow CT
There is a known discrepancy between the anatomic severity of coronary stenosis and physiology. Assessing coronary flow (or pressure) is essential for determining risk and making clinical decisions using both noninvasive and invasive methods.28 Recommendations emphasize the significance of conducting invasive physiologic evaluation during ICA in symptomatic patients with a high-risk clinical profile and of contemplating revascularization for enhancing angina in patients with persistent symptoms despite optimal medical treatment. Several studies have demonstrated that utilizing FFR to guide PCI improves patient outcomes, underscoring the importance of physiological assessment. Computational fluid dynamics and image-based modeling techniques have been developed to compute vessel-specific FFRCT values from data obtained during CCTA scans. FFRCT allows for the computation of pressure differences in the coronary arteries, offering a physiological evaluation of CAD, and aiding in clinical decisions for myocardial revascularization.29
FFRCT mainly focuses on evaluating lesion-specific physiology to assist in deciding whether to refer for invasive angiography and has been proven to enhance efficiency in the catheterization lab by raising the PCI/ICA ratio.30 The available data allows for the potential integration of factors like lesion location, extent of physiological disturbance, and translesional gradient into the planning of PCI. Individuals with narrowings in certain areas of the coronary arteries may experience a significant decrease in pressure. In contrast, those with widespread coronary artery disease may have a small and consistent reduction in pressure throughout the vessel, particularly in the distal segments. It is essential to note that the physiological phenotype cannot be distinguished from the angiographic anatomy. While both situations result in irregular heart artery function, the possible revascularization results vary significantly.31
The FFR pullback maneuver can assess the distribution of epicardial resistance based on pressure loss magnitude and functional disease extent. Anatomically widespread CAD is frequently treated with optimal medical therapy or coronary artery bypass graft (CABG) in a conservative approach.32 While the effectiveness of PCI in widespread CAD is uncertain, restoring blood flow to specific coronary narrowings with abnormal FFR values enhances physiological functioning and reduces ischemia.33 A recent examination of the ADVANCE registry showed that adding the delta FFRCT or translesional gradient enhances the differentiation of patients who had early revascularization, as opposed to the standard CCTA with FFRCT diagnostic approach. Randomized trials mandated binary cutpoints for revascularization decisions, but analysis of extensive registry data revealed a correlation between lower FFR values and increased risk of future clinical events.34 Furthermore, greater enhancement in FFR post-PCI results in increased symptom relief and reduced incidence of vessel-oriented clinical events. Despite lacking a thorough understanding of the potential mechanisms involved, it is believed that diffuse CAD is often responsible for limited improvement in FFR following revascularization. Cardiologists need to be aware of this discovery and adjust their treatment plan to achieve the most favorable clinical result35 (Figure 1).
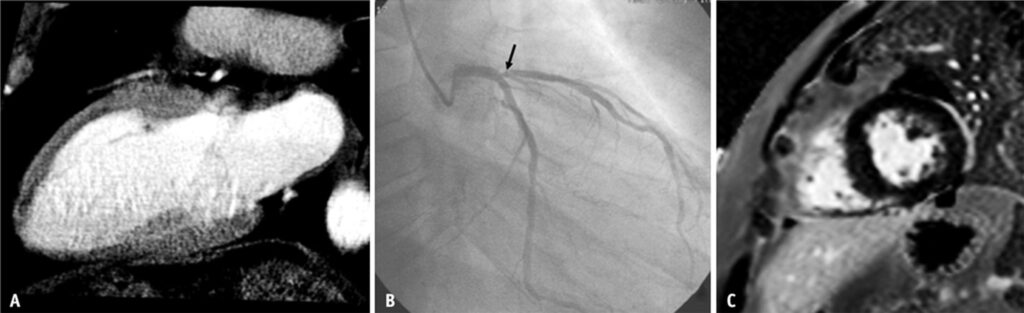
(A) Coronary CT angiography source images revealed a non-transmural perfusion defect in the subendocardium within the LAD territory through static CT perfusion assessment.
(B) The proximal segment of the supplying artery (LAD) exhibited a 70% stenosis (arrow) with a fractional flow reserve (FFR) value of 0.72, confirming the lesion as functionally significant.
(C) Six months after coronary intervention, a late gadolinium-enhanced short-axis MR image of the middle left ventricular wall showed no myocardial infarction involving the anterior wall. CT = computed tomography, LAD = left anterior descending.36
Different Role of CTP and FFRCT
Coronary CT perfusion (CTP) and CT-derived fractional flow reserve (FFRCT) fulfill different yet complementary functions in evaluating coronary artery disease (CAD). Both methods utilize noninvasive imaging to yield essential insights into coronary physiology and hemodynamics, although each emphasizes a distinct aspect of disease evaluation.
Coronary CT Perfusion (CTP) seeks to view and evaluate myocardial perfusion, or blood flow inside the cardiac muscle, offering a direct assessment of ischemia areas (Figure 2).
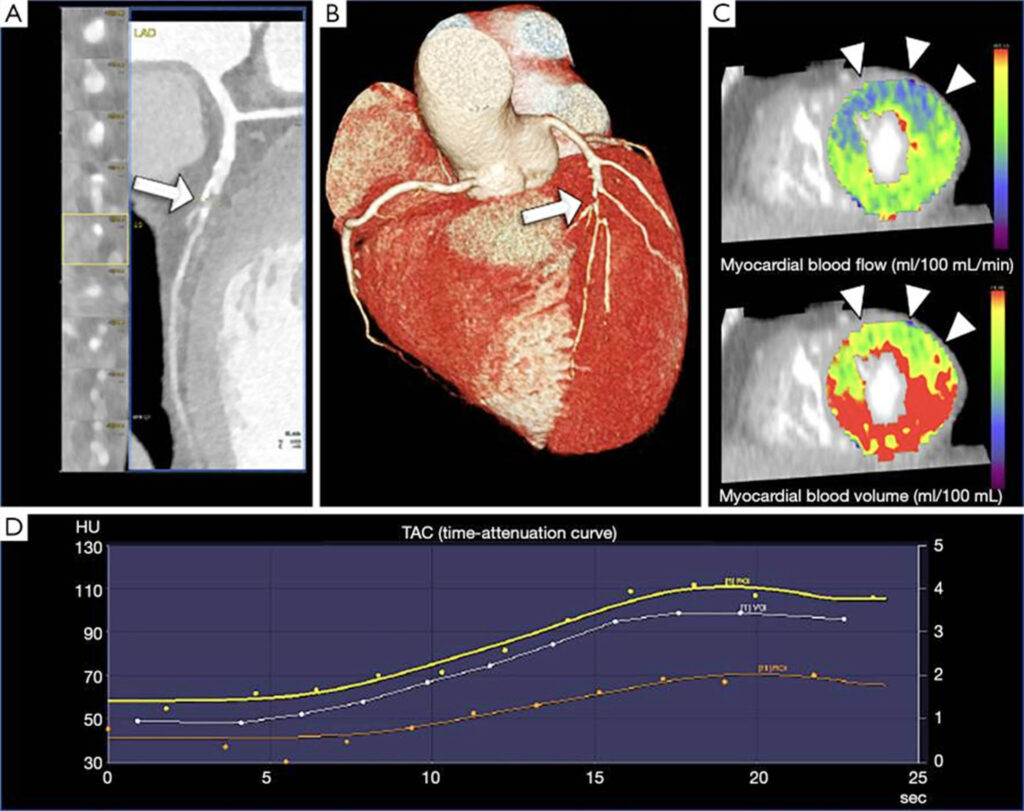
This method use contrast-enhanced CT imaging, sometimes combined with pharmacologic stress agents such as adenosine, to assess the adequacy of blood flow to various regions of the myocardium. CTP delineates ischemic zones, especially in instances of intermediate or severe stenosis, by revealing diminished perfusion areas under stress or at rest. This information is crucial for assessing the severity of cardiac ischemia, which may dictate revascularization choices. CTP assists doctors in detecting ischemia territories, enabling them to target regions that may benefit from care, hence enhancing patient outcomes by concentrating on locations with the greatest risk of adverse effects.38, 39
In contrast, CT-derived Fractional Flow Reserve (FFRCT) provides an indirect measure of blood flow limitation across coronary stenoses by estimating the pressure gradient. Unlike CTP, FFRCT does not directly image perfusion within the myocardium. Instead, it uses computational fluid dynamics applied to standard coronary CT angiography (CTA) images to predict the pressure drop across specific lesions. This technique estimates the fractional flow reserve, a ratio of distal to proximal pressure under simulated maximal blood flow conditions, allowing clinicians to gauge whether a coronary lesion is likely to cause ischemia. FFRCT is particularly useful for assessing the hemodynamic significance of intermediate lesions (40–70% stenosis), often guiding whether a patient should proceed to invasive angiography or revascularization. By indicating which lesions are functionally significant, FFRCT can reduce unnecessary interventions and support evidence-based treatment planning.40, 41
CTP and FFRCT together provide a thorough evaluation of coronary artery disease (CAD). CTP assesses myocardial perfusion to detect ischemic areas, while FFRCT provides information on the physiological effects of coronary stenosis. This amalgamation improves decision-making for patients with CAD, facilitating a more customized approach to treatments.42, 43
CONCLUSION
The chance to utilize CCTA technologies and advanced analytics is facilitating the shift of CCTA from solely a diagnostic tool to one that can be utilized for planning coronary interventions. Further research is required to fully investigate how CCTA can enhance catheterization lab efficiency, increase revascularization success, and improve patient outcomes.
REFERENCES
1. Zhou Z, Xu L, Zhang N, Wang H, Liu W, Sun Z, Fan Z. CT coronary angiography findings in non-atherosclerotic coronary artery diseases. Clin Radiol. 2018;73(2):205-213. CrossRef Pubmed
2. Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, et al. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020 Jan 14;41(3):407-477. CrossRef Pubmed
3. Li SY, Zhong J, Qiao HY, Schoepf UJ, Emrich T, Butler WN, Zuo R, Xue Y, Liu Y, Dai LY, Zhou CS, Lu GM, Tang CX, Zhang LJ. FFR CT and Static Computed Tomography Myocardial Perfusion Imaging for Therapeutic Decision-making and Prognosis in Patients With Coronary Artery Disease. J Thorac Imaging. 2024 Mar 1;39(2):101-110. doi: 10.1097/RTI.0000000000000718. Epub 2023 May 22. PMID: 37265250; PMCID: PMC10878454. CrossRef Pubmed
4. Chen J, Wetzel LH, Pope KL, Meek LJ, Rosamond T, Walker CM. FFRCT: Current Status. AJR Am J Roentgenol. 2021;216(3):640-648. CrossRef Pubmed
5. Zito A, Galli M, Biondi-Zoccai G, Abbate A, Douglas PS, Princi G, et al. Diagnostic Strategies for the Assessment of Suspected Stable Coronary Artery Disease: A Systematic Review and Meta-analysis. Ann Intern Med. 2023;176(6):817-826. CrossRef Pubmed
6. Bangalore S, Toklu B, Patel N, Feit F, Stone GW. Newer-Generation Ultrathin Strut Drug-Eluting Stents Versus Older Second-Generation Thicker Strut Drug-Eluting Stents for Coronary Artery Disease. Circulation. 2018; 138 (20): 2216 – 2226. CrossRef Pubmed
7. Stone GW, Christiansen EH, Ali ZA, Andreasen LN, Maehara A, Ahmad Y, et al. Intravascular imaging-guided coronary drug-eluting stent implantation: an updated network meta-analysis. Lancet. 2024; 403(10429): 824-837. CrossRef Pubmed
8. Pergola V, Pradegan N, Cozza E, Cozac DA, Cao I, Tessari C, et al. Redefining CAV surveillance strategies: Benefits of CCTA vs. ICA. J Cardiovasc Comput Tomogr. 2024; S1934-5925(24)00392-7. Pubmed
9. Andrew M, John H. The challenge of coronary calcium on coronary computed tomographic angiography (CCTA) scans: effect on interpretation and possible solutions. Int J Cardiovasc Imaging. 2015;31 Suppl 2:145-57. CrossRef Pubmed
10. Laksono S, Maya Suryana N. The Role of Coronary CT Angiography in Chronic Total Occlusion Coronary Intervention. Int J Cardiovasc Pract. 2024; 9(1): e145138. CrossRef
11. Hang K, Zhao G, Su W, Bao G, Zhao Q, Jiao Z, et al. Coronary artery-to-pulmonary artery fistula in adults: evaluation with 320-row detector computed tomography coronary angiography. Ann Transl Med. 2021; 9(18): 1434. CrossRef Pubmed
12. de Araújo Gonçalves P, Campos CA, Serruys PW, Garcia-Garcia HM. Computed tomography angiography for the interventional cardiologist. Eur Heart J Cardiovasc Imaging. 2014; 15(8): 842-54. CrossRef Pubmed
13. Sharma RK, Arbab-Zadeh A, Kishi S, Chen MY, Magalhães TA, George RT, Dewey M, Rybicki FJ, Kofoed KF, de Roos A, Tan SY, Matheson M, Vavere A, Cox C, Clouse ME, Miller JM, Brinker JA, Arai AE, Di Carli MF, Rochitte CE, Lima JA. Incremental diagnostic accuracy of computed tomography myocardial perfusion imaging over coronary angiography stratified by pre-test probability of coronary artery disease and severity of coronary artery calcification: The CORE320 study. Int J Cardiol. 2015 Dec 15;201:570-7. doi: 10.1016/j.ijcard.2015.05.110. Epub 2015 May 19. PMID: 26334382. CrossRef Pubmed
14. Rief, M., Zimmermann, E., Stenzel, F., Martus, P., Stangl, K., Greupner, J., Knebel, F., Kranz, A., Schlattmann, P., Laule, M., & Dewey, M. (2013). Computed tomography angiography and myocardial computed tomography perfusion in patients with coronary stents. Journal of the American College of Cardiology, 62(16), 1476–1485. https://doi.org/10.1016/j.jacc.2013.03.088 CrossRef Pubmed
15. Antonopoulos AS, Angelopoulos A, Tsioufis K, Antoniades C, Tousoulis D. Cardiovascular risk stratification by coronary computed tomography angiography imaging: current state-of-the-art. Eur J Prev Cardiol. 2022;29(4):608-624. CrossRef Pubmed
16. Laksono S, Hosanna C, Angkasa IS. Clinical Characteristic Findings From Coronary CT Angiography in Patients With Chronic Coronary Syndrome. Cardiovasc Imaging Asia. 2024; 8: e2. CrossRef
17. Laksono S, Prawara AS and Kusharsamita H. Cardiac computed tomography and its use in clinical practice: a review. Iberoam J med. 2023; 5(3): 123-134. CrossRef
18. Eckert J, Schmidt M, Magedanz A, Voigtländer T, Schmermund A. Coronary CT angiography in managing atherosclerosis. Int J Mol Sci. 2015;16(2):3740-56. CrossRef Pubmed
19. Johnson TW, Räber L, di Mario C, Bourantas C, Jia H, Mattesini A, et al. Clinical use of intracoronary imaging. Part 2: acute coronary syndromes, ambiguous coronary angiography findings, and guiding interventional decision-making: an expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur Heart J. 2019;40(31):2566-2584. CrossRef Pubmed
20. Czaja-Ziółkowska M, Głowacki J, Krysiński M, Gąsior M, Wasilewski J. Relationship between left main trifurcation angulation, calcium score, and the onset of plaque formation. Kardiol Pol. 2023;81(1):48-53. CrossRef Pubmed
21. Alyami B, Santer M, Seetharam K, Velu D, Gadde E, Patel B, Hamirani YS. Non-Calcified Coronary Artery Plaque on Coronary Computed Tomography Angiogram: Prevalence and Significance. Tomography. 2023 Sep 20;9(5):1755-1771. CrossRef Pubmed
22. Lorenzatti D, Piña P, Huang D, Apple SJ, Fernandez-Hazim C, Ippolito P, Abdullah A, Rodriguez-Guerra M, Skendelas JP, Scotti A, Kuno T, Latib A, Schenone AL, Nasir K, Blankstein R, Blaha MJ, Berman DS, Dey D, Virani SS, Garcia MJ, Slipczuk L. Interaction between risk factors, coronary calcium, and CCTA plaque characteristics in patients aged 18-45 years. Eur Heart J Cardiovasc Imaging. 2024 Jul 31;25(8):1071-1082. CrossRef Pubmed
23. van Driest FY, Bijns CM, van der Geest RJ, Broersen A, Dijkstra J, Scholte AJHA, Jukema JW. Utilizing (serial) coronary computed tomography angiography (CCTA) to predict plaque progression and major adverse cardiac events (MACE): results, merits and challenges. Eur Radiol. 2022;32(5):3408-3422. CrossRef Pubmed
24. Monizzi G, Sonck J, Nagumo S, et al. Quantification of calcium burden by coronary CT angiography compared to optical coherence tomography. Int J Cardiovasc Imaging 2020; 36 (12): 2393 – 2402. CrossRef Pubmed
25. Wang YH, Chen WJ, Chen YW, et al. Incidence and Mechanisms of Coronary Perforations during Rotational Atherectomy in Modern Practice. J Interv Cardiol 2020; 1894389. CrossRef Pubmed
26. Williams MC, Kwiecinski J, Doris M, et al. Low-Attenuation Noncalcified Plaque on Coronary Computed Tomography Angiography Predicts Myocardial Infarction: Results from the Multicenter SCOT-HEART Trial (Scottish Computed Tomography of the HEART). Circulation 2020; 141(18): 1452 – 1462. CrossRef Pubmed
27. Purwowiyoto, S. CT-FFR: Clinical Application. Indonesian Journal of Cardiology 2018; 39(1), 50-54. CrossRef
28. Chen J, Wetzel LH, Pope KL, Meek LJ, Rosamond T, Walker CM. FFRCT: Current Status. AJR Am J Roentgenol. 2021;216(3):640-648. CrossRef Pubmed
29. Huang AL, Maggiore PL, Brown RA, Turaga M, Reid AB, Merkur J, Blanke P, Leipsic JA. CT-Derived Fractional Flow Reserve (FFRCT): From Gatekeeping to Roadmapping. Can Assoc Radiol J. 2020;71(2):201-207. CrossRef Pubmed
30. Douglas PS, Pontone G, Hlatky MA, et al. Clinical outcomes of fractional flow reserve by computed tomographic angiography-guided diagnostic strategies vs. usual care in patients with suspected coronary artery disease: the prospective longitudinal trial of FFR(CT): outcome and resource impacts study. Eur Heart J 2015; 36 (47): 3359 – 3367. CrossRef Pubmed
31. Collet C, Sonck J, Vandeloo B, et al. Measurement of Hyperemic Pullback Pressure Gradients to Characterize Patterns of Coronary Atherosclerosis. J Am Coll Cardiol 2019; 74(14): 1772 – 1784. CrossRef Pubmed
32. Dourado LOC, Bittencourt MS, Pereira AC, et al. Coronary Artery Bypass Surgery in Diffuse Advanced Coronary Artery Disease: 1-Year Clinical and Angiographic Results. Thorac Cardiovasc Surg 2018; 66 (6): 477 – 482. CrossRef Pubmed
33. Piroth Z, Toth GG, Tonino PAL, et al. Prognostic Value of Fractional Flow Reserve Measured Immediately After Drug-Eluting Stent Implantation. Circ Cardiovasc Interv 2017; 10(8): e005233. CrossRef Pubmed
34. Al-Lamee R, Howard JP, Shun-Shin MJ, et al. Fractional Flow Reserve and Instantaneous Wave-Free Ratio as Predictors of the Placebo-Controlled Response to Percutaneous Coronary Intervention in Stable Single-Vessel Coronary Artery Disease. Circulation 2018; 138(17): 1780 – 1792. CrossRef Pubmed
35. Bom MJ, Schumacher SP, Driessen RS, et al. Non-invasive procedural planning using computed tomography-derived fractional flow reserve. Catheter Cardiovasc Interv 2021; 97 (4): 614 – 622. CrossRef Pubmed
36. Yun CH, Hung CL, Wen MS, Wan YL, So A. CT Assessment of Myocardial Perfusion and Fractional Flow Reserve in Coronary Artery Disease: A Review of Current Clinical Evidence and Recent Developments. Korean J Radiol. 2021 Nov;22(11):1749-1763. doi: 10.3348/kjr.2020.1277. Epub 2021 Aug 19. PMID: 34431244; PMCID: PMC8546143. CrossRef Pubmed
37. Seitun S, Clemente A, De Lorenzi C, Benenati S, Chiappino D, Mantini C, Sakellarios AI, Cademartiri F, Bezante GP, Porto I. Cardiac CT perfusion and FFRCTA: pathophysiological features in ischemic heart disease. Cardiovasc Diagn Ther. 2020 Dec;10(6):1954-1978. doi: 10.21037/cdt-20-414. PMID: 33381437; PMCID: PMC7758766. CrossRef Pubmed
38. Pontone G, Andreini D, Guaricci AI, et al. Stress Computed Tomography Perfusion: A New Tool to Optimize the Diagnostic Workflow of Patients With Ischemic Heart Disease. J Am Coll Cardiol. 2018;71(22):2565-2576.
39. Berman DS, Schussheim Role of Myocardial Perfusion Imaging in the Era of CT Angiography and Fractional Flow Reserve CT. Eur Heart J. 2020;41(5):903-911.
40. Koo BK, Erglis A, Doh JH, et al. Diagnosis of Ischemia-Causing Coronary Stenoses by Noninvasive Fractional Flow Reserve Computed from Coronary Computed Tomographic Angiograms. J Am Coll Cardiol. 2011;58(19):1989-1997. CrossRef Pubmed
41. Nørgaard BL, Leipsic J, Gaur S, et al. Diagnostic Performance of Noninvasive FFR Derived from Coronary CT Angiography in Suspected Coronary Artery Disease: The NXT Trial. J Am Coll Cardiol. 2014;63(12):1145-1155. CrossRef Pubmed
42. Gould KL, Johnson NP, et al. Anatomic Versus Physiologic Assessment of Coronary Artery Disease: Role of Coronary Flow Reserve, Fractional Flow Reserve, and Positron Emission Tomography Imaging in Revascularization Decision-Making. J Am Coll Cardiol. 2013;62(18):1639-1653. CrossRef Pubmed
43. Patel MR, Califf RM, et al. One-Year Results of a Randomized Trial of Fractional Flow Reserve–Guided Versus Angiography-Guided PCI. N Engl J Med. 2019;380(13):1288-1297.
Copyright Information